Here’s what dawned on me: What if this same process — breaking down, metabolising, and regenerating — is exactly what needs to happen with our relationships, our identities, our trauma, our inherited beliefs?
What if transformation isn’t about releasing your pain or transcending your trauma… but about metabolising it? Composting it into the soil that grows your authentic life?
That’s a different question from the one most wellness frameworks are answering.
Most of what’s out there is catharsis. Cry it out. Let it go. Release. Transcend. Heal your inner child. And look — catharsis is real. The relief is real. But here’s what took me forty years to understand: catharsis and metabolisation are not the same thing.
The Difference That Changes Everything
You can cry in every session and still walk out into the same patterns.
You can shout it out, shake it out, breathe it out, pray it out — and three months later, find yourself back at the same crossroads. A different face, a different address, but the same dynamic. The same choice. The same moment of recognition that something fundamental hasn’t shifted.
Catharsis asks: ‘How do I release this?’
Metabolisation asks: ‘What does this become?’
Your cells don’t just expel damaged proteins. They break them down, recover amino acids and building blocks, and use those recovered materials to synthesise new, healthy structures. The damage becomes resource, the wound wisdom. The dysfunction that was killing you becomes the very material from which you build something your lineage has never had before.
That’s Dimensional Autophagy.
Not releasing. Not transcending. Not bypassing. Metabolising.
The Inheritance Nobody Asked For
I left home at 17. Moved five hours away, from isolation to what I thought was a possibility. I didn’t go home for years. I thought I’d cleared the patterns. Put distance between me and the dysfunction. Created space for something new.
At 19, I walked straight from my family’s patterns into a marriage driven by religious shame. Same dysfunction. Different postcode. Because here’s what I hadn’t understood yet: you can’t clear geography and call it healing. The patterns weren’t in the location. They were in my whakapapa, in me.
I was carrying obligations that weren’t mine. Loyalty patterns from generations back. Roles I’d never chosen but had somehow become responsible for. And on top of all of that, I was carrying something I didn’t even have a name for yet: colonial PTSD.
The Wound with Three Names
Colonisation isn’t just history. It’s a complex trauma — and for Māori, and for many indigenous and displaced peoples, it presents with a specific pattern I’ve come to call the three exiles.
The First Exile: The original displacement. Land. Language. Identity. Spiritual practice. The severing of whakapapa connection through the mechanisms of colonisation. This isn’t a metaphor. This is the literal loss of the web of relationships that make you who you are.
The Second Exile: The double exile. You navigated a Pākehā world for decades and survived it by becoming something in between. Not white enough to fully belong. Not Māori enough to return. Forty-one years of corporate life of code-switching, of being told your ‘brand’ needed changing — when what was happening was the systematic dismantling of who you were. Deconstruction of Identity – you became a Brown Pākehā. You didn’t choose it. It was done to you, incrementally, in the name of professional development.
The Third Exile: The exile of the displaced. When you finally tried to come home, your own people didn’t recognise you. Urban migration and cultural disconnection had made you strange to your whakapapa. The door that should have opened didn’t. This is perhaps the most devastating exile of all, because it strips you of the homecoming you’ve been reaching for.
Colonisation is Poison Ivy. It spreads beneath the surface, invisible and symptomless, until one day it erupts as a crisis. If you don’t know it’s there, you treat the rash. You don’t find the root.
The anxiety, depression, identity fragmentation, relational chaos — these aren’t personal failures. They’re the eruptions of an unmetabolised colonial wound, and the wound has an origin that is not you.
The foundational reframe of this entire framework is this:
You can only give what you were given. You pass on what you know.
That’s not an excuse for harm. It’s a restoration of dignity. It puts the wound back where it began — outside you — so you can deal with it.
What Dimensional Autophagy Actually Is
Dimensional Autophagy applies the cellular autophagy process — breakdown, metabolisation, regeneration — to five core dimensions of human experience within Te Poutama Ora, a nine-dimensional Māori wellness framework.
The five dimensions where trauma most deeply accumulates are these:
• Whakapapa (Relational/Genealogical) — The toxic patterns you inherited. The obligations that aren’t yours. Relational dynamics running from generations back that you somehow became responsible for carrying forward.
• Wairua (Spiritual) — The false beliefs, religious shame, and spiritual bypassing. The disconnection from an authentic encounter with Te Ao Wairua, Te Atua, that happened when the framework given to you couldn’t hold your actual life.
• Tuakiri (Identity) — The false self-created to survive. Code-switching, performance realignment. The colonial conditioning that made you small, acceptable, non-threatening. And the rage you were never allowed to feel about any of it.
• Hinengaro (Mental/Emotional) — The thought loops. The anxiety has been trying to tell you something for years. The depression that is not a pathology but a closing down in the face of impossible situations.
• Tinana (Physical) — The body that holds everything. All the relational wounds, spiritual disconnection, identity fractures, and emotional material that never found its way out. Your body is the final archive.
What This Work Is Not
Let me be clear, because there’s enough spiritual bypassing masquerading as healing in the wellness world.
• This is not ‘just let it go.’
• This is not magical thinking or toxic positivity.
• This is not a requirement to confess every secret or perform your trauma publicly.
• This is not therapy, and it doesn’t replace it.
• This is not for people in acute crisis — stabilisation comes first.
This is transformation through lived and resolved experience. Teaching from the other side of the wound, not from inside it.
Specifically: this is metabolisation, not catharsis. You will not be invited to relive your trauma repeatedly until it loses emotional charge. You will be guided through structured breakdown, metabolisation, and regeneration — one dimension at a time — until what was destroying you becomes the very material you build from.
When the Pattern Won’t Shift: Te Wetekina, The Loosing
There’s something that happens in this work that nobody talks about honestly enough.
You do the recognition work. You name the pattern. You can see exactly what you’re doing and why it doesn’t serve you, and then you do it again anyway.
This is not a failure of discipline. This is not a lack of commitment. This is a stronghold.
You cannot break a stronghold with willpower.
Strongholds are different from ordinary habits. Ordinary habits shift through awareness, intention, and consistent practice. Strongholds resist because they entered through a specific door — a moment of wounding, a survival decision, a pattern handed to you through your whakapapa — and that door has never been intentionally closed. The pattern has roots deeper than behaviour. It entered through a covenant, and an altar was established. Until that altar is dismantled, the pattern has a home.
Te Wetekina — the loosing — is the practice of finding that door. Naming the moment it opened. Understanding what covenant was made, what was promised and what was actually delivered. Then, consciously and with spiritual authority, dismantle the altar and replace the covenant with something that serves your mana.
I know this from the inside. During my own Whakapapa Autophagy work, I was trying for weeks to break a pattern of alcohol use on weekdays. Boundaries were in place. Intentions clear. I kept returning to it — same time, same pull, same moment. Then I understood: this wasn’t just my habit. Alcohol abuse was a pattern across generations in my whakapapa. I had been introduced to it through manipulation at a specific moment I could identify. An altar had been established in my ancestral line long before me. No amount of willpower was going to close a door that had been open for generations.
The action I took was Te Wetekina: I identified the precise moment the stronghold made its bid each day, and I built a specific karakia practice — invoking divine intervention at that moment, every time. Not in a general way. At that exact time. At that exact trigger. I upped my practice of the Inoi a te Ariki, invoked te Atua’s intervention every time the thought surfaced, and thanked God every time I resisted.
The next morning, I woke feeling different. Like I had crossed generations.
That is Te Wetekina. Not just personal healing — genealogical healing. The closing of a door that had been open in your whakapapa for longer than you’ve been alive. It threads through the Whakapapa, Wairua, and Tuakiri dimensions of the autophagy work specifically — wherever strongholds have established themselves through inherited covenant, spiritual wounding, or identity assault.
Because it requires the engagement of Te Ao Wairua as co-agent — because the authority to dismantle an altar is spiritual, not merely psychological — it names something that most Western frameworks leave unnamed: that some healing requires divine covenant to complete.
Walking Through the Five Dimensions
Whakapapa Autophagy: What’s Not Yours to Carry
Four generations of healing work in my whakapapa. My grandfather was an Anglican minister. My grandmother was forced to practice healing underground. My father, a founding member of Men for Change in the 1980s, was working with men from prison on domestic violence. I am developing Te Poutama Ora—my adult children, carrying that same orientation into law enforcement, education and psychology.
What I had to learn is that the healers in a lineage also carry the wound. Being the strong one, the fixer, the one who holds it together — that’s not just a calling. It’s sometimes an inherited obligation that was never examined. Whakapapa autophagy is about knowing the difference.
It’s not about cutting people off. It’s not about abandoning your whānau. It’s about recognising which patterns are yours and which were handed to you before you were old enough to choose. Then, with full respect for the lineage that transmitted them, putting those obligations down.
When a pattern in your whakapapa won’t shift — when you can see it clearly and return to it anyway — that’s when Te Wetekina enters. Because some of what you’re carrying isn’t just an inherited habit. It’s an ancestral altar, and altars need to be consciously dismantled, not just walked away from.
Wairua Autophagy: Finding What Was Always There
I was unshakeable in my Christian faith as a child. By my mid-twenties, it had become silent. Not because faith is wrong, but because the version I’d been given was received through a colonial political mechanism, not as a living encounter. When my actual life — the complexity, the pain, the choices — arrived, the framework couldn’t hold it.
What I’ve come to understand, after years in cave seasons, my site of praxis, is what I now call the Whakapapa Dilemma: the experience of feeling like a spiritual impostor when your genealogical identity doesn’t trace to the Abrahamic covenant. The feeling that you have no legitimate spiritual ground to stand on.
The resolution wasn’t theological. It was lived. The recognition that the sacred was present through all of it — through every cave season, every spiritual death, every desperate reaching. “God had me all that time. I had covered my own eyes.”
Wairua autophagy clears the shame-driven beliefs, the religious trauma, the spiritual bypassing. It makes space for an authentic encounter — whatever form that takes for you.
It is here, in the wairua dimension, that Te Wetekina finds its deepest ground. Because when a spiritual stronghold is present — a belief, a shame, a door that was opened in the spirit and never intentionally closed — the clearing requires more than insight. It requires divine authority. The karakia is not decoration. It is the mechanism through which the loosing happens.
Tuakiri Autophagy: Reclaiming What Was Taken
Forty-one years in white-collar environments. They told me they were changing my brand, dismantling me. Systematically. In the name of professional development.
The Brown Pākehā experience is specific: you survive by becoming something in between. Not quite yourself, not quite them, and because you were good at it, because you could code-switch fluently enough, nobody named what was happening. It looked like success. It felt like disappearing.
Tuakiri autophagy is rage work. It’s the anger you weren’t allowed to feel for forty years. It’s naming what was done to you rather than what you did wrong. It’s composting the performance self — not with grief for it, but with recognition that it served its purpose and is no longer needed.
Then it’s standing in cultural identity without apology. Not performing Māori-ness. Being it, on your own terms, without asking anyone’s permission.
Hinengaro Autophagy: Listening to the Messenger
In my first marriage, I believed I was failing because I wasn’t good enough. The truth was the marriage was toxic, and my hinengaro was trying to tell me exactly that. Through anxiety, depression, and isolation. Through the desperation of not wanting to pass this on to another generation.
My mental and emotional patterns weren’t the problem. They were messengers.
Here’s the thing that changed everything for me: “You can’t think your way out of patterns created by relational trauma, spiritual shame, and identity assault”. That’s why Hinengaro comes fourth in the programme.
First, you clear the whakapapa, the wairua, the tuakiri. Then the hinengaro naturally follows. Because it was never the primary wound. It was the symptom of the primary wound.
Tinana Autophagy: The Body Remembers, and the Body Releases
My body has ‘died’ twice. Breast cancer, twice. Two serious illnesses that forced spiritual rebirth.
I thought my body was betraying me. Now I understand: my body was doing the clearing my mind couldn’t yet comprehend. The body keeps the score of everything that hasn’t been metabolised. Every relational pattern, every spiritual wound, every identity fracture, every emotional loop that never found its way out.
Tinana comes last because you can’t fully clear physical patterns while carrying the accumulation of the other four dimensions. But once you’ve done that dimensional work — once the whakapapa, wairua, tuakiri, and hinengaro have been metabolised — the body responds in ways that would have been impossible before.
Fasting isn’t just physical. It’s the final composting of everything you’ve metabolised across all dimensions.
The Healing Instrument: Taha Auaha
The ninth dimension of Te Poutama Ora is Taha Auaha — Creative Wellness. It works differently from all the others.
Taha Auaha is not a container. It’s the healing instrument through which metabolisation becomes real in your body, your life, your relationships. It’s what the experience becomes when it’s been broken down and transformed.
The rage becomes a poem. The grief becomes a song. The fracture becomes a story that helps someone else find their way. The wound becomes the teaching.
This is not art therapy as an add-on. This is the understanding that human beings metabolise through making — and that Māori have always known this. Waiata, haka, tukutuku, kōrero: the creative was never separate from the healing. We separated them.
Taha Auaha brings them back together.
How the Programme Works
Dimensional Autophagy runs across five months — one dimension each month. The sequence matters. The architecture supports the work.
Each month moves through four phases:
• Te Tūāhuatanga (Recognition) — Seeing the pattern clearly. Naming its origin. Refusing the shame that has kept it invisible.
• Te Kāwhatitanga (Breakdown/Clearing) — Beginning the intentional dissolution. Naming what needs to go. Sitting in the discomfort of that recognition.
• Te Whakahuatanga (Metabolisation) — Staying in the material long enough to extract wisdom. Composting the toxin. Letting the dysfunction become teaching.
• Te Tuku (Release/Integration) — Releasing what cannot be carried forward. Integrating what has been transformed. Moving forward has changed.
Each dimension is engaged through the Tūāpapa trinity: Recognition, Reclamation, Restoration. You see it. You take back what was taken. You build what was never there.
The teaching tools — the monthly workbooks — carry you through this process with structured practices, release protocols, integration work, and daily practices. They’re built for people ready to do real work, not looking for comfort.
Who This Is For
This work is for you if:
• You’re exhausted by every other method you’ve tried.
• You can feel the patterns running, but can’t find the off switch.
• You suspect the wound you’re carrying started before you did.
• You’re done with spiritual bypassing, toxic positivity, and being told to ‘just let it go.’
• You want to metabolise your trauma, not transcend it.
• You’re ready — not perfect, not healed, but ready.
This work is not for you if you’re looking for quick fixes, magic healing, or someone to rescue you. This is your work. Through guidance and holding space, you learn what you need to metabolise that deep wound.
The Invitation
Your body already knows how to do this. At the cellular level, every single day, it breaks down what’s damaged, metabolises what can be learned, and regenerates what’s healthy.
What if you could do the same with your whakapapa? Your beliefs? Your identity? Your trauma? Your patterns?
Not by transcending them. Not by performing recovery. Not by pretending any of it didn’t happen.
By metabolising it. Composting it. Transforming it into the soil that grows your authentic life.
That’s what your whakapapa has been waiting for. That’s what your lineage — four generations, five generations, ten generations back — has been reaching toward. Not the passing on of what they couldn’t release. But the creation, finally, of what was never there.
When I am tau, te Ao Mārama is tau. When I am settled, the world is settled. This is the work.
About the Author
Ruku I’Anson is a crisis and wellness counsellor, and founder of Te Poutama Ora — a nine-dimensional Māori wellness framework developed from lived and resolved experience and four generations of healing lineage. Ruku teaches from 41 years of lived experience in corporate environments, and hard-won wisdom about what it takes to metabolise trauma into transformation. For more, visit Iantemo.com.
These are the feelings we all face at some stage in our lives. The internet only makes it worse, now we compare ourselves to others daily. We are bombarded by the posts of others’ success.
Maybe we can partly blame evolution for this feeling. We’re naturally inclined to feel dissatisfied or to be driven towards finding more satisfaction in life so that we will keep moving forward, doing the things that help us survive and succeed (Veenhoven, 1996; Kageyama & Sato, 2021).
Note: If you would like to just learn the strategies you can skip to “How to Stop Feeling like a Failure.” Otherwise read on to understand the theory behind these feelings.
Problem 1: You’re focused on everyone else.
Maybe you’re thinking, “I really am a failure, I’m not succeeding in life, everyone else is doing so much more”. What standards are you measuring yourself by?
Take your standard and go through this list of people to decide who is a success and who is a failure:
A 5 month old baby who hasn’t uttered a word.
A student who failed their exam
A person who makes $40k a year
A 30 year old who lives with their parents
How did you do? Was anyone neither? Maybe you thought, there’s not enough information here to make that decision?
Now if you compare yourself to these people, how are you doing? I believe, compared to the baby, you’re doing quite well because you’re reading this post.
“Why would I compare myself to a baby”
Why not compare yourself to a baby? I imagine it’s because they’re at a different stage of life.
But we all are.
There is not a single person on Earth who you can fairly compare yourself to because the different environments and circumstances we experience places us at different stages. When we’re born, we’re not put on the same starting line.
Problem 2: These thoughts are given power.
Maybe it feels hopeless and like you’re subjected to challenges that others don’t have. Challenges that you have no control over. It’s true, there are many things in life we cannot control.
The only two things forever in our control are how we think and how we act. Do you agree?
We can’t ask people to stop posting their achievements online which makes us feel bad. But we can change our thoughts when we see those posts (or we can take action by uninstalling social media).
For some people, they probably know where this is going and they don’t want to hear it. “I’m tired of people telling me to just think positive.”
I get it and I don’t want to do just that (in fact, in this post I’ve listed a few different approaches so that maybe you’ll find something that feels right for you).
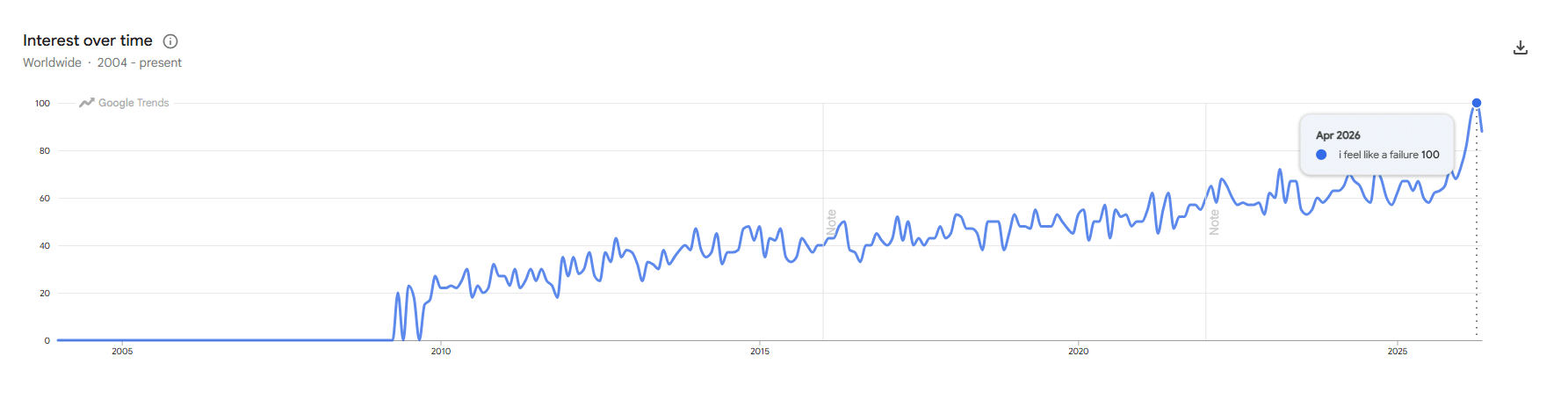
I’m not going to say the answer to your lifelong misery is to “just think positive”. If it were that easy, the google searches for “I feel like a failure” wouldn’t look like this:
22k searches over the last month…How is it that so many of us feel like a failure.
Some might feel resistant to the idea of looking inwards at their thoughts and feelings, maybe it makes you cringe, or it feels uncomfortable.
I understand looking inwards can feel like “airy, fairy, yoga nonsense.” You’ve probably heard the terms “mindfulness”, “gratitude” and “just think positively” too many times and meditation never worked for you. But science backs up the power our thoughts have over us.
A review of more than 4,000 studies involving over 500,000 participants found that positive psychology activities (changing your thoughts towards positive thinking) can help reduce anxiety, stress, depression and improve overall wellbeing (Carr et al., 2024). That’s a whole lot of research pointing in the same direction
Again, these negative feelings are partly an evolutionary response to motivate us to keep moving forward. For some of us, it works out, but for those googling “I feel like a failure”, it might feel like you’re being dragged down rather than forward.
Negative feelings become a problem when they overwhelm you and make it harder to get out of bed in the morning. These feelings can be really hurtful, breaking down your self-esteem and sense of self (Mulawarman et al., 2025).
How to Stop Feeling Like a Failure
The answer seems like it would be simple: just start achieving. Maybe you’ve tried this and it feels good for a while but then that feeling creeps back in… You do more and more but it seems like you can’t catch a break for long.
Problem 3: The problem hasn’t changed.
You’ve slapped a bandaid on top, a temporary fix. Or maybe you’ve developed another workaround to cope, or avoid it…as much as you can. You haven’t yet addressed the root of the problem: the negative thoughts. What if you changed how you think?
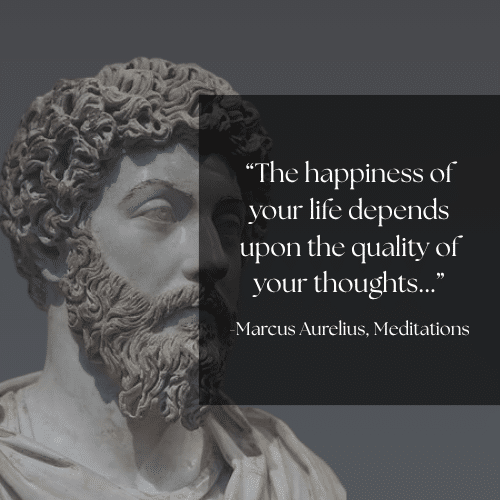
Many of the world’s most famous thinkers (philosophers) believed this was the answer to handling the ups and downs of life.
Remember: The two things in our lives we have control over are how we think and act.
You can’t get your friends to stop talking about their achievements but you can change what you think when you hear them.
There is no magic tool, resource or treatment that will change your thinking in an instant. It takes patience and time to retrain yourself out of the negative thinking patterns you’ve developed in response to your past environments.
Psychology has developed many ways of addressing your negative thoughts. Although Cognitive Behavioural Therapy (CBT) is regarded as the most effective therapy in Psychology, when it comes to our unique minds, there is no one-size-fits-all approach. So I have listed a variety of ideas from different therapies that may help.
If one approach doesn’t work for you, don’t give up; try out another technique.
Cognitive Behavioural Therapy (CBT)
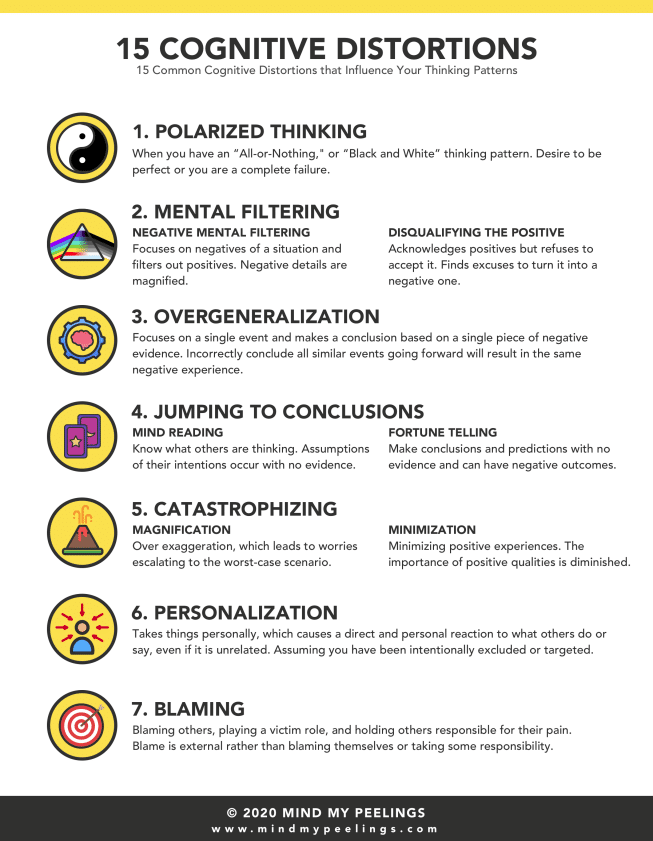
Our thoughts are not always fact. Some people develop a lens that distorts reality, leading to negative thinking. For example, situations like going to a party may make you feel dread because you assume the worst will happen. CBT names this as the Fortune Telling distortion. Do you recognise any of the below cognitive distortions in your own thinking:
Learning to identify your cognitive distortions when they appear is the first step. Next is to turn it into a habit and learn to challenge your thoughts. Here’s a video to help:
If you are finding it difficult to identify your cognitive distortions, talking with a therapist might help.
Acceptance and Commitment Theory
When we compare our lives to those of others, we may begin to lose sight of ourselves. You may pick up goals that don’t truly align with your values. So one place to start may be rediscovering yourself and your values. Here are two videos to help you start:
ACT also teaches something called Cognitive Defusion. It’s about creating space from your difficult thoughts and feelings. When that thought “I feel like a failure” is at the front of your mind, it can be really hard to get past it and do anything. This is where the Cognitive Defusion technique may be useful:
CFT recommends you to start treating yourself like a friend. Feeling shame and punishing yourself only creates more damage, struggle, and makes it harder to feel motivated to do anything. Be self-compassionate. If you feel like you’re struggling with being overly critical towards yourself, you might like this:
If you want to explore this further, a compassion-focused trained therapist can help you.
Solution-Focused Brief Therapy (SFBT)
For those who don’t find looking inward helpful. Try solution-focused therapy or ask yourself solution-focused questions that redirect your thinking away from the problems and negative thoughts:
What makes you feel like you’re ahead in life?
What makes you feel good?
When do you feel proud of yourself?
When do you feel like you’re doing well?
Build Back Your Self-Esteem, Self-Confidence and Your Sense of Self
Part of not feeling like a failure, and not feeling the need to compare yourself to others, comes from self-esteem. Self-esteem is about self-love, how you value yourself and how confident you feel in who you are.
What makes self-esteem so important?
Imagine this scenario: You’re wearing your normal everyday clothes. Now, a stranger walks up to you and says: “That’s a stupid pink unicorn outfit, you look really silly in that.”
What’s your reaction?
I imagine it might be disbelief and confusion. You’re not wearing a pink unicorn outfit? What is this crazy person on about…Instead of internalising it and becoming self-conscious, you just think they’re wrong, and they’re the ones who must be confused.
How do you begin to treat all scenarios like this one?
One place to start may be relearning who you are and what you love. You can’t be confident in yourself if you don’t know yourself. Here are some ideas to help you rediscover yourself:
Spend time with yourself and be present. Journal to record your inner thoughts, or maybe take a walk on your own and just let yourself think.
For another take on finding yourself, I highly recommend watching this video, it explains the story of Po from Kung Fu Panda.
This is a story remembered for training hard and believing in yourself. But the story goes deeper. It’s actually the story of accepting who you are and that you need to let go of this ideal/perfect version of yourself that you’re trying to be:
The word gratitude can feel overused or like cheap, low-effort advice. But there is real science behind the importance of gratitude.
It directly counteracts negative feelings in your brain. It sounds too simple but things like gratitude journaling can really help to change the way you think, for the better. Regular gratitude practice can gradually change the way we interpret situations by shifting our attention toward positive aspects of life (Kini et al., 2016).
Gratitude is the reason some people with very little can still find contentment.
Check out this video to learn more about gratitude:
Take one photo of something you appreciate each day
Pay It Forward – Share something you have with someone else (food, shelter, skills, knowledge)
Gratitude Jar – Every time you think of something you are grateful for, put it on a strip of paper into a jar. When you need to be reminded of what you are grateful for, take one from the jar
Explore philosophy
If you’re a very intellectual, curious person or you just love learning you might like this. Many philosophies have great teachings that can help us learn to love ourselves and to let go. Here are some examples that may interest you:
Carr, A., Finneran, L., Boyd, C., Shirey, C., Canning, C., Stafford, O., … & Burke, T. (2024). The evidence-base for positive psychology interventions: A mega-analysis of meta-analyses. The Journal of Positive Psychology, 19(2), 191-205.
Kageyama, J., & Sato, K. (2021). Explaining the U-shaped life satisfaction: Dissatisfaction as a driver of behavior. Journal of Bioeconomics, 23(2), 179-202.
Kini, P., Wong, J., McInnis, S., Gabana, N., & Brown, J. W. (2016). The effects of gratitude expression on neural activity. NeuroImage, 128, 1-10
Mulawarman, M., Antika, E. R., Hariyadi, S., Miftachul‘Ilmi, A., Prabawa, A. F. I., Benu, K. M., … & Lathifah, A. A. (2025, April). The Influence of Positive Self-Talk on Students’ Self-Criticism: a Cross-Sectional Study. In The 8th International Conference on Education Innovation (ICEI 2024) (pp. 811-818). Atlantis Press
Veenhoven, R. (1996). The study of life-satisfaction.
Te Poutama o te Ora — the framework I’d been building for some time now — has nine steps. I walked through those steps, took notice of what came up, what parts were easy and some not so.
My goal for my Tinana Dimension was “I will only drink water with dinner”. My practice activity and boundary became “No alcohol Monday to Friday”. Clear, measurable, and — I can tell you — genuinely difficult. The first week was a grind. I’d got to Wednesday, and after a successful workday, I thought “I’ll have a glass of wine with dinner”. Ah yes….but then there was my Tinana goal, and the commitment I had made. I was glad when Friday came. When it got to the following Monday, I found I had made sure there was no wine in the house, so I had no excuses or temptations. Monday came and went without drama.
Omutu
I track the maramataka phases every week in ‘Taku Maramataka”, a planning and guidance tool I designed that situates you in the Cosmo. I didn’t notice it immediately; however, I traced that I had just shifted into the phase of Omutu under Whiro’s influence, the Autumn phase of the month. A time to fast, detox and retreat. And, it all made sense. I was fasting in the right phase and rhythm of the month.
With this realisation and the physical boundary of “no wine in the house” in place, the fast was easier. I took notice of my thoughts as the days continued. Incredibly, I weighed less, and then a calming sense of control came over me. I put a second boundary in place – eat meals at home; going out to dinner or lunch only once a month. Then I realised after a few weeks that we hadn’t bought takeaway food…happy pocket-$$$…happier weight.
Reading the Map That Was Already There
The Maramataka names every night of the lunar month. Each night has its own character, its own invitation. Some nights are for planting. Some are for fishing. Some are for gathering. Some are for rest. This isn’t mythology — it’s an ancient observational system built over generations of watching how the natural world actually behaves in relationship to the moon.
And looking at those names through the lens of the nine steps, I could see it: the programme’s first step — Te Ohorere, the awakening, the moment when you first decide to change — belonged at Mawharu. The first reach of the waxing moon. The natural moment of beginning.
Once I saw that, everything else followed. Each step found its natural home in the lunar month. Reflection fell where the moon was full and clear. Release work fell where the moon was waning. Rest and integration fell in the dark of the new moon. The programme wasn’t something I was imposing on the Maramataka — it was something the Maramataka had been holding, waiting to be seen.
Ninety Days
When I mapped the full journey, it took three complete moon cycles to walk all nine steps through to integration. Three cycles. Roughly ninety days.
That number started appearing in other places. Habit researchers talk about 66 days on average for a new behaviour to stick. Many recovery programmes use 90 days as a meaningful threshold. But what struck me was that in this case, 90 days wasn’t arbitrary. It wasn’t an estimate or a convention. It was the time the Maramataka required.
Three full turnings of te marama. A complete journey.
What If You Start Mid-Cycle?
The next practical question was obvious: not everyone can start at the same time. What happens if someone comes to the programme in the middle of a moon cycle?
The answer reshaped everything. What matters is not that everyone starts together — it’s that each person starts at their own Mawharu. The next waxing moon that arrives for them.
Their own moment of beginning.
From that insight came the Three Rhythms — three simultaneous cohorts, each beginning at a different Mawharu, each following the same path. The programme is always running. There’s no waiting for the next intake. There’s just the next moon.
Te Aho Maramataka — The Thread
I eventually built what I call Te Aho Maramataka — a guide that maps each of the nine TPO wellness dimensions to the four lunar phases.
Waxing for growth and new practices. Full moon for expression and celebration. Waning for releasing what no longer serves. New moon for rest, stillness, and quiet intention-setting.
It’s not a rigid protocol. It’s a navigation compass. A way of asking: what phase are we in, and what does this moment call for?
Each of the nine dimensions — identity, relationships, mental and emotional wellbeing, spirituality, physical health, digital wellness, food and gut health, finances, creativity — has its own relationship to each phase. The guide makes that visible.
Why This Matters
Most wellness programmes are built on the assumption that time is neutral. That a Monday in March is the same as a Thursday in October. That the only thing that matters is the intervention itself — the exercises, the worksheets, the sessions.
But if you’ve ever tried to make a significant change in your life, you’ll know that time isn’t neutral. There are moments when growth feels effortless. There are moments when release comes naturally. There are moments when you genuinely need to rest, not push.
The Maramataka has been tracking those moments for generations. Te Poutama o te Ora is a programme that listens to that tracking.
The Wednesday I struggled, the realisation that came on the following Monday as I moved into Omutu, was the shift, and not a coincidence. It was a body responding to the natural rhythm of Te Taiao – the environment. And what the 90-Day Engine does, at its heart, is design a programme that honours that relationship rather than ignoring it.
I return again to my post about “Today’s Alignment” that uses the Maramataka and TPO Rhythm experience. The Maramataka is calibrated to Whiro, the new Moon and the beginning phase of the lunar calendar.
If you missed that article, you are warmly invited to explore the live experience here and join the community:
Te Poutama o te Ora is a nine-dimensional kaupapa Māori wellness framework developed in Aotearoa New Zealand. With Taha Tuakiri — identity and purpose — at its centre, TPO guides individuals and communities through a structured journey toward holistic wellbeing, using the Maramataka as its temporal spine. The 90-Day Engine and Te Aho Maramataka are core programme tools within the TPO suite.
Maramataka — the rhythmic thread that weaves through all dimensions.
The word Maramataka comes from two Māori words: marama (moon, month, understanding) and taka (to turn over, to change). Together they describe a system of knowledge rooted in the idea that life moves in cycles — and that tuning into those cycles is both a practical and a spiritual act.
The Maramataka is not just a lunar calendar. It is a living archive that brings together knowledge of the stars, the sea, the soil, and the seasons. It tracks ecological signs — the flowering of certain plants, the behaviour of birds and fish, the temperature of the wind — and uses them to guide human activity. Different iwi (tribal communities) kept their own regional versions of the Maramataka, adapted to the land and water systems they called home.
When colonisation suppressed the Māori language, land use, and cultural practice, the Maramataka was among the knowledge systems pushed underground. Its revitalisation today is not simply about tradition for tradition’s sake. It is about reclaiming a profound and practical intelligence — one that contemporary science is increasingly recognising as valid.
Te Poutama o te Ora — A Framework That Breathes
Te Poutama o te Ora (TPO) is built across nine dimensions of wellbeing. At its centre stands Taha Tuakiri — the Pou of identity and cultural wellness — because the work has always held that you cannot flourish in any other dimension of life if you are not grounded in who you are. From that centre, eight further dimensions radiate outward: Taha Tinana (physical), Taha Hinengaro (mental and emotional), Taha Wairua (spiritual), Taha Whānau (relational), Taha Kai (nutritional), Taha Pūtea (financial), Taha Matihiko (digital), and Taha Auaha (creative).
These nine dimensions do not exist in isolation. They breathe together, and what gives them their shared rhythm — what ties them to the living world and to each other across time — is the Maramataka.
TPO is a stairway. The nine dimensions are its Pou — the carved posts that hold the structure upright. The Maramataka is the central thread that weaves from Te Tūāpapa – the Foundation to Te Ao Marama – Full Flourishing, connecting every Pou, giving alignment and direction. Without this thread, the interconnectedness of Te Poutama is not in cohesive rhythm…a set of dimensions without a when.
When I am tau — settled and in rhythm — te Ao Mārama is tau.
The world of light reflects the peace within.
The Four Phases: A Rhythm for Living
The Maramataka divides the lunar month — roughly 29.5 days — into a sequence of named nights, each with its own character and guidance. For those new to the system, these are often introduced as four broad phases. Think of them like the seasons within each month.
In TPO, each phase creates a natural cadence for how we engage with the nine dimensions.
🌘The Waxing Moon — Te Marama Tupu
This is the moon building toward fullness — the time of rising energy. In the garden, this is when you plant and sow. In life, it is the time to begin that project, make that call, schedule that hard conversation. Your body is in a building phase — anabolic, growing, energised.
In TPO terms, the waxing phase is the prime window for Taha Tinana — physical training and building practice. It is also the moment to activate Taha Pūtea (financial planning and new income moves) and Taha Matihiko (launching digital projects, engaging new platforms). Taha Auaha stirs here too — this is when creative energy is available, and it asks to be used.
🌕 The Full Moon — Te Marama Kaha / Te Rākaunui
Peak energy. Peak light. This is the time the Maramataka traditionally reserved for large community gatherings, harvests, and ceremonies. It is when the landscape is most visible, when fish are most active near the surface, when collective energy is highest. Sleep may be lighter than usual around this phase — that is not a failure, that is the moon.
The full moon is the natural home of Taha Whānau within TPO — the relational dimension that asks us to show up for our people and receive them in return. It is also the moment when Taha Tuakiri comes alive in the community: identity is not only an inner experience but also confirmed and celebrated in the presence of those who know your name and your lineage. Plan your gatherings, your celebrations, your deep conversations here.
🌘 The Waning Moon — Te Marama Hinga / Tangaroa
The moon begins its return to darkness, and the invitation is to follow. This is the best phase for fishing (certain species were understood to be more active as tidal patterns shift), and it is the ideal time for therapeutic work, rest, reflection, and letting go.
In TPO, the waning moon is the natural rhythm for Taha Hinengaro — the mental and emotional wellness dimension. This is when we process, integrate, and release. It is the therapeutic window: the phase where clinical work lands most deeply, where journalling opens, where the body is ready to let go of what it has been carrying. Taha Wairua deepens here too — spiritual practice moves inward, prayer and reflection finding their natural ground.
🌑 The Dark Moon — Te Marama Mate / Ōmutu
This is the still point before renewal — the most spiritually significant phase in the Maramataka. Physical activity is discouraged. This is the time to go inward: to tend to whakapapa, to rest deeply, to prepare for what comes next.
In TPO, the dark moon is sacred to Taha Wairua and Taha Tuakiri in their most interior forms. It is also, quietly, a Taha Kai moment — the body’s natural fasting window, a time for clearing and cleansing. Practitioners working within TPO use this phase to review, to sit with supervisors, to let the previous cycle settle before the next one begins. It is not empty time. It is the soil being prepared.
Rest is not what you earn after doing enough. It is what the Maramataka says you need — built into the rhythm of every month.
The Maramataka and the Nine Dimensions — A Living Alignment
This is not a rigid prescription. The Maramataka does not divide life into sealed compartments — it offers a rhythm of emphasis. Each dimension is alive in every phase. But the following mapping offers a practitioner’s guide to where each dimension finds its fullest expression across the lunar cycle:
🌘Waxing Moon
Taha Tinana (Physical Wellness) → Building, training, and new health practices
Taha Pūtea (Financial Wellness) → New income activity, planning, financial decisions
Taha Matihiko (Digital Wellness) → Launching, creating, digital engagement
Taha Auaha (Creative Wellness) → Beginning creative projects, generating new work
🌕 Full Moon
Taha Whānau (Relational Wellness) → Gathering, celebrating, communal connection
Taha Tuakiri (Identity Wellness) → Cultural celebration, whakapapa, community affirmation
Taha Auaha (Creative Wellness) → Sharing, performing, presenting creative work
🌘 Waning Moon
Taha Hinengaro (Mental/Emotional Wellness) → Therapeutic work, processing, integration
Taha Wairua (Spiritual Wellness) → Deepening spiritual practice, prayer, reflection
Taha Auaha (Creative Wellness) → Refining, editing, completing creative cycles
🌑 Dark Moon
Taha Wairua (Spiritual Wellness) → Deep rest, ancestral connection, stillness
Taha Tuakiri (Identity Wellness) → Inner whakapapa work, identity renewal
Taha Kai (Nutritional Wellness) → Fasting, cleansing, preparing the body for renewal
Taha Auaha — creative wellness — moves with special freedom across all four phases, because creative practice is both the instrument and the expression of every other dimension. It plants in the waxing, blooms at the full, processes in the waning, and rests in the dark. This is why, within TPO, Taha Auaha is understood not merely as a dimension but as a healing instrument that moves across the whole framework.
Why This Matters for Wellness
Food and Growing
The Maramataka’s guidance for planting and harvesting according to lunar phases is not folklore — it is ecological intelligence. Biodynamic farming research has now validated the principle that lunar gravitational influence affects soil moisture and plant growth. In TPO, Taha Kai is not simply about what we eat — it is about our relationship with food as a source of mauri, a carrier of whakapapa, a measure of tino rangatiratanga. Community māra kai guided by the Maramataka are a living expression of that relationship.
Physical Health
Contemporary chronobiology — the science of the body’s internal rhythms — tells us that our physiological performance, immune function, and recovery capacity all fluctuate in patterns that extend well beyond the 24-hour clock. TPO’s Taha Tinana has always known this. Its differentiation between high-energy phases and restorative phases gives practitioners a culturally grounded template for periodising exercise, therapeutic interventions, and workload guidance that serves both client and clinician.
Mental and Spiritual Wellbeing
Perhaps the Maramataka’s greatest contribution to modern wellness is its insistence that spiritual and relational wellbeing are not optional add-ons to health — they are foundational. This aligns with Durie’s Te Whare Tapa Whā model, and with TPO’s positioning of Taha Tuakiri at the centre of the whole framework. The Maramataka doesn’t just suggest you make time for these things. It tells you when. That is the gift of a temporal spine.
The Maramataka in the Digital Age
One of the more exciting developments in recent years is the emergence of digital Maramataka tools — apps and platforms that make this guidance accessible to urban Māori communities who may be far from traditional knowledge holders, and to younger generations who engage first with the world through their phones. Within TPO, Taha Matihiko asks us to reclaim digital space as a site of Māori wellness — not to be consumed by the algorithm, but to use technology in service of tino rangatiratanga. A Maramataka-guided digital tool is one expression of that reclamation.
But this comes with an important caution. The Maramataka is not wellness content to be packaged and sold. It is a living, community-embedded knowledge system that belongs to Māori. Any digital platform that carries the Maramataka must be developed and governed by Māori knowledge holders, in accordance with the principles of indigenous data sovereignty. When that is done well, the digital Maramataka is not a diluted version of the real thing — it is a new expression of it.
The TPO 90-Day Engine: From Awareness to Authority
What makes the Today’s Alignment tool more than a daily check-in is the architecture running underneath it: the TPO 90-Day Engine — a complete wellness journey built directly into the bones of the Maramataka.
Three rhythms run simultaneously, each cycling through nine steps from beginning to end. Every rhythm starts at the same place: Mawharu — the star associated with new beginnings — with Step 1, Te Ohorere: Awareness. Every rhythm ends at the same place: Huna, with Step 9, Te Whakamana i tō Mana — Reclaiming Authority. Ninety days. Nine steps. The full arc of the journey, from first noticing to standing fully in your own power.
The genius of the three-rhythm structure is that at any given night of the Maramataka, someone is always at a different stage of the journey. Because the three rhythms are staggered across the lunar cycle, you can enter the programme wherever the moon finds you — and the rhythm places you exactly where you are ready to begin. The engine doesn’t wait for you to start at the beginning. It recognises something the Maramataka has always known: real movement begins where you are, not where the calendar says you should be.
This is what Taha Matihiko looks like in practice — not technology imposed on wellness, but technology shaped by it. The Today’s Alignment tool is the Maramataka’s temporal intelligence made visible and portable, carrying the 90-Day Engine wherever you go.
Coming Home to Rhythm
There is something quietly revolutionary about the Maramataka in a world that tells us to be constantly productive, always on, endlessly optimising. It says: no. There is a time for expansion and a time for rest. A time for harvest and a time for fasting. A time for gathering and a time for silence.
That is not a limitation. It is a liberation.
Within Te Poutama o te Ora, the Maramataka is the temporal spine of the whole framework — the rhythm that runs through every one of the nine dimensions, from Taha Tinana to Taha Auaha, from the body’s daily needs to the soul’s seasonal hungers. It is not one component among many. It is what makes all the other dimensions coherent.
Whether you are a practitioner, a community member, or simply someone trying to live a little more in tune with the world around you, the Maramataka offers something that very few modern wellness systems can: a way of knowing when.
When I am tau — when I am settled and in rhythm — te Ao Mārama is tau. The world of light reflects the peace within.
If you read the introduction to Today’s Alignment, you will be using the Maramataka and TPO Rhythm experience.
If you missed that article, you are warmly invited to explore the live experience here and join the community:
As a child, my Christian faith was unshakeable. God was real. The Bible was the truth. I didn’t question.
By my mid-twenties, it had all crumbled. Not because faith is wrong, but because the version I’d been given couldn’t hold the complexity of my actual life — my choices, my pain, and the truth as a Māori person navigating a world that had been shaped to accommodate someone else’s story.
I carried a secret for 40 years. Not because anyone was forcing me, but because religious shame was so deeply internalised I couldn’t even name it to myself.
But the shame wasn’t only about what I’d done or not done. It went deeper than that. It went all the way to whakapapa.
The Question That Wouldn’t Leave Me
Here is the dilemma I could never quite name, but always felt:
“How can I be Christian when I don’t whakapapa back to God’s people? I’m not Jewish.”
I knew my whakapapa. On my mother’s side, I trace back to Porourangi — the great ancestor from whom Ngāti Porou descend. On my father’s side, to Rangatira Momo, the ancestor of Te Momo. These are ancient, living, sovereign lines. These are my people.
But when I opened the Bible, I found a story that began with Abraham and flowed through a lineage I had no genealogical connection to. The God of scripture had made his covenant with a specific people. I was not one of those people.
And the Christianity I’d received? It hadn’t arrived as a gift. It had arrived with a flag. The Anglican ministry given to me as a child was deeply rooted in England’s political agenda — a tool used to reshape those they colonised, to create compliant subjects rather than liberated souls. I knew this. My bones knew this.
So I felt like an impostor. I was worshipping in a tradition that wasn’t mine, delivered by a power that had harmed my people, built on a genealogy I couldn’t trace.
That feeling is its own kind of trauma. It doesn’t look like the obvious wounds — not shame about your body, not fear of hell, not the memory of religious leaders who hurt you. It’s quieter than that. It’s the constant, low-level hum of wondering whether you belong.
When Religion Becomes a Weapon
Religious trauma happens when spirituality gets weaponised for control:
• Your body is sinful
• Your sexuality is shameful
• Your questions are dangerous
• Your Māori spirituality is demonic
• Your culture is primitive
• You are not of the covenant people
These aren’t spiritual truths. They are wounds masquerading as theology.
For Māori who were raised in colonial Christianity, the wound is compounded: you were handed a faith and simultaneously told — implicitly and sometimes explicitly — that the culture you came from made you less suited for it. You had to become more like the messenger to be eligible for the message.
That is violence. And naming it as violence is not rejecting God. It is being honest about what human beings did with God’s name.
The Dilemma: Three Options
When you see this clearly, you face what seems like three impossible options:
Option 1: Stay in the toxic faith as you received it, performing belief in a tradition you know was weaponised.
Option 2: Reject Christianity entirely and return exclusively to te ao Māori spiritual frameworks.
Option 3: Find a third way.
I couldn’t do Option 1. I’d seen too clearly. And I couldn’t do Option 2 either — because despite everything, my encounters with God were real. The faith in my bones wasn’t performative. It was mine.
So I had to find the third way. And that third way wasn’t a compromise — it turned out to be the original truth, buried under centuries of colonial distortion.
The Cave That Changed Everything
I didn’t find my way through by thinking it…I was driven through it.
When redundancy came, I lost the thing I’d been using to avoid the question: the financial stability, the corporate identity, the altar I’d built to security.
Taylor Welch talks about a process that began to make sense of what happened to me. He describes it as movements through which purpose-driven people pass, and the ‘Cave’ became my site of praxis:
• Crisis: You know change is needed. You take no action. You maintain the false altar.
• Consecration: You are forced to face it. The altar is removed. You find yourself in a cave — isolated, hidden, refining. This is costly. This is also where the real work happens.
• Confrontation/Clash: What was created in the cave begins to meet the world. People want what you have. But life is still awkward. You are still in survival mode. The remnants are being shaped.
• Multiplication: Things finally take off. The refined work finds its scale.
• Institutionalisation: The remnants are packaged and shared on a stage. The story becomes a legacy.
I was made redundant. I was isolated. I felt like I was in a cave — hiding, dark, uncertain, and it was in that cave that Te Poutama o te Ora emerged. The thinking I’d suppressed for decades came flooding out. The questions I’d been too busy to ask demanded answering.
And one of those questions was the oldest one: Am I really God’s?
What I Found in the Cave
I am still somewhere between the Consecration and Confrontation stages as I write this.
TPO is still being shaped. The books are still being written. Two part-time jobs add up to more than 53 hours a week. Religious study fills the remaining hours. Life is full and demanding, and not yet arrived.
But I know something now that I didn’t know before the redundancy. Or rather, I believe something I used to only argue about.
God did not leave me in that cave. He was in the cave with me, and the theology that had made me feel like an impostor was the theology of the colonial church, not the theology of the New Covenant.
Here is what I found:
The New Covenant through the blood of Jesus Christ is not an ethnic inheritance. It is not for Jews only. It is for all whakapapa. Paul writes in Galatians that in Christ there is neither Jew nor Greek — and that all who belong to Christ are Abraham’s seed, not through genealogy, but through promise.
In the logic of the New Covenant, belonging is not determined by birth into the right people. It is determined by the blood that covers every person.
My Porourangi whakapapa is not cancelled by my faith.
My Te Momo whakapapa is not superseded by the cross.
They are held alongside it. I belong to both, and they do not fight each other.
The impostorship was never real. It was a colonial lie.
God had me all that time. I had covered my own eyes. Matapihi Kirihou o Nga Karu.
Releasing the Shame, Keeping the Wisdom
Through the process of wairua autophagy — the nine-cycle framework at the heart of Te Poutama o te Ora — I’ve been learning to metabolise what was toxic and keep what is true.
That means:
• Naming the colonial church as a political instrument without rejecting the faith it distorted
• Honouring my Māori whakapapa without treating it as incompatible with covenantal belonging
• Acknowledging the impostor feeling as a trauma response, not a theological verdict
• Finding God in the cave, not as a reward for surviving it, but as the one who was present in it
• Understanding that my place in the covenant does not require me to stop being Māori
You are Not an Impostor
If you are Māori — or from any indigenous people — and you carry this quiet ache, this sense that the faith you hold is somehow borrowed, somehow not properly yours — I want to say something clearly:
The colonial church was not God. It was people using God’s name. What they gave you was a distorted package. The faith inside the package is real, and it was never only for Jewish people.
Your whakapapa is not a disqualification. It is not an obstacle. It is the line God has always known.
The covenant through Christ does not require you to become someone else. It invites you, as you are, from the whakapapa you carry, into a belonging that no colonial agenda was ever authorised to gatekeep.
The Autophagy of Dimension Programme
The full Autophagy of Dimension programme through Te Poutama o te Ora addresses wairua (spiritual) trauma across nine cycles over five months. It is designed for people navigating:
• Colonial religious trauma and the Whakapapa Dilemma
• Shame-based faith and fear-based theology
• The impostor experience in spiritual identity
• The integration of te ao Māori and Christian spirituality
You don’t have to choose between your whakapapa and your faith. You don’t have to perform a belief that doesn’t hold your full complexity.
Release the shame. Keep the wisdom. Come home to who you actually are.
Here’s what I’ve learned, both from developing Te Poutama o te Ora and from working with people in my practice: the method matters far less than the match. A habit-building approach that energises one person creates invisible friction for another. Not because of commitment levels. Not because of willpower. But because of orientation, the natural way each person tends to move through a process.
Today I’m going to introduce you to the Three Orientations, help you figure out which one you are, and then show you which of the three practice methods I recommend for your 18-day Kaha cycle. One method. Yours. For 18 days.
Let’s go.
First — What’s a Nine-Day Cycle Got to Do with It?
Within TPO, Step 2 Whakatūria tō Mana Establishing your Authority is structured as two consecutive nine-day cycles. With a brief pause between cycles. This isn’t arbitrary. Nine days is long enough for genuine neurological rewiring to begin — the kind that changes behaviour — and short enough that you can hold focus and motivation across the whole arc. Two cycles give you the chance to consolidate what you started in the first, and to deepen from ‘I’m doing this’ into ‘this is part of who I am.’
But here’s the thing. Not everyone experiences those three phases equally. Some of us come alive at the beginning and start to drift by Day 6. Some of us need a little running start, but then hit our stride in the middle. Some of us only really relax into it when the finish line is in sight.
That’s not a character flaw. That’s orientation.
The Three Orientations
◈ The Starter
You’re energised by new beginnings. The moment when a project or practice is just getting started — when it’s all possibility and no problems yet — is where you feel most alive. You’re great at overcoming inertia, generating ideas, and making the first move. Your challenge? Once the path is set and the work becomes repetitive, your attention can start to drift toward the next exciting beginning.
Your method: Anchor New Practices to Existing Routines
💡 Design your anchors on Day 1 (this is genuinely fun for you). Let the existing routine carry you through Days 4–9 when novelty fades. On Day 10, you get a legitimate refresh — a small redesign moment to keep you engaged.
◈ The Middler
You thrive in the doing. Give you some structure to work within, a bit of direction, and enough latitude to navigate your own way — and you’ll keep going long after others have stopped. The long middle of any project is your natural home. Your challenge? Blank-page beginnings can feel nebulous, and the final details of completion can feel constraining.
Your method: The 3-Tier Integration System
💡 You write your own content into the three tiers (this suits your self-directed style). The framework gives you something to push against without locking in the outcome. Tier 3 has built-in grace for days when life interrupts — no guilt, no shame, just keep going.
◈ The Finisher
You’re animated by completion. You see the gap between ‘nearly done’ and ‘actually done’ that everyone else seems to minimise — and closing that gap is where you come alive. You’re patient, meticulous, and capable of real sustained focus once momentum is building. Your challenge? Starting from zero can feel overwhelming because you can’t yet see what you’re finishing.
Your method: Simple Daily Tracking
💡 The tracker gives you a visible finish line every single day — exactly what your motivational system needs. Setting it up on Day 1 gives you just enough clarity to begin. By Day 18, you’ll have two full weeks of visible evidence. That will feel deeply satisfying. Because it is.
Not Sure Which One You Are? Try This Quick Quiz
Answer each question honestly — not the person you want to be, but the person you recognise. There are no wrong answers.
1. When you start something new, you feel most…
A. Excited. This is the best part.
B. Ready — once there’s a bit of structure to work with.
C. Confident — once I can see what ‘done’ looks like.
2. By Week 2 of any new habit or programme, you tend to…
A. Be eyeing off the next interesting thing.
B. Be in your stride and feeling solid.
C. Be frustrated that you can’t yet see the finish line.
3. The part of the 18-day cycle that will be hardest for me is…
A. Days 7–9. Closing out and completing.
B. Days 1–3. Getting started.
C. Days 1–6. Before I can see the end.
4. When I miss a practice day, I’m most likely to…
A. Start fresh with a whole new approach.
B. Review, adjust, and keep going.
C. Feel unsettled until I’ve ticked something off.
5. My natural strength in this 18-day journey will be…
A. Designing the practice and committing early.
B. Sustaining momentum through the long middle.
C. Completing every entry and finishing strong.
📊 Your result
Mostly A → You’re a Starter. Your method: Anchor New Practices to Existing Routines. Mostly B → You’re a Middler. Your method: The 3-Tier Integration System.
Mostly C → You’re a Finisher. Your method: Simple Daily Tracking.
Mixed? Ask yourself: which phase of a project tends to feel most alive for you? That’s your orientation.
One Method. 18 Days. That’s It.
I want to be clear about this: you are not being asked to use all three methods. Just one. The one that matches your orientation.
This is intentional. One of the most common reasons people fall off a new practice programme isn’t lack of motivation — it’s cognitive overload. Too many systems running at once creates a management problem on top of a habit problem. You end up spending your energy tracking the systems instead of living the practice.
One method, chosen well, is enough. It’s more than enough. It’s sustainable.
🌿 A note on mana
Choosing your own method — rather than being assigned one — is itself an act of mana. Self-determination theory tells us that when we choose something because it genuinely fits us, we’re far more likely to sustain it than when we follow something prescribed from outside. This small act of self-knowledge at the start of your 18 days is part of building Kaha. It’s not a preliminary step. It is the step.
What Happens at the End of 18 Days?
At the end of your two cycles, I’ll be asking you to sit with a few reflection questions:
• Which phase of the cycle felt most alive for you?
• Which phase felt most like resistance?
• What did your method make easier — and what did it not quite hold?
This isn’t about whether you ‘succeeded.’ It’s about what you learned about yourself. Because that self-knowledge becomes the foundation for Steps 4–6, where we start to deepen and integrate across multiple dimensions of wellbeing.
You’re not just building a habit. You’re building a relationship with your own nature. And that, friends, is where real Kaha comes from.
Over to You
Take the quiz. Identify your orientation. Choose your method. Commit to it for 18 days.
And if you want to share — which orientation resonated with you, and which method you’re going with — drop it in the comments or send me a message. I love hearing how people see themselves in this work.
The academic companion article to this blog — Orientation-Responsive Practice Selection: Matching Method to Person in the 18-Day Kaha Cycle — explores the research base behind this approach, including habit formation theory, self-determination theory, and the neurological basis of the nine-day cycle. Available on request.
The self-diagnostic tool is also available as a formatted stand-alone document for use in individual practice or group settings.